Thalidomide
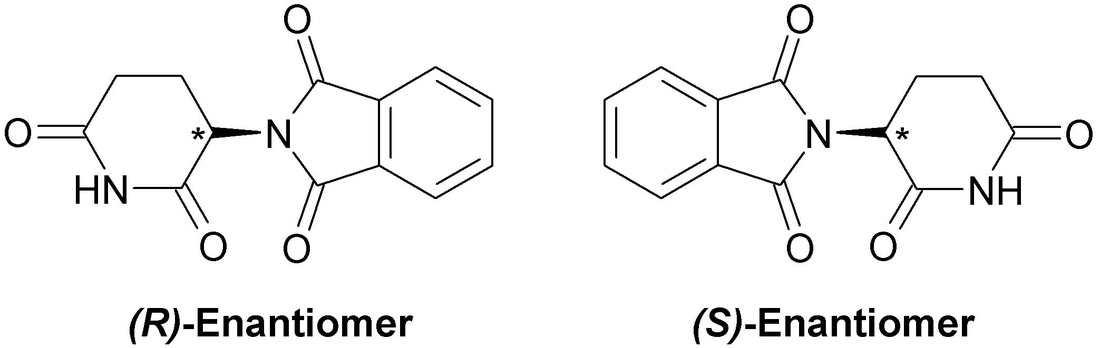
The 'S' enantiomer is teratogenic while 'R' enantiomer exhibits no developmental toxicity. However the molecules will racemise within in vivo condition, therefore toxicity will occur even if R enantiomer administered only.
WONDER DRUG
In 1957 German pharmaceutical company Chemie Grünenthal began marketing thalidomide, proclaiming it as a “wonder-drug” for the treatment of multiple ailments including insomnia, seizures, headaches, and later as an anti-nauseant. The drug initially appeared highly safe, with few side effects and low risk of overdoes relative to other sedatives available at the time. Researchers found the drug was particularly effective as an antiemetic and many pregnant women began taking thalidomide to alleviate their morning sickness. By 1959 an estimated one million people were taking thalidomide on a daily basis in Germany and its use was extensive in 45 other countries across Europe, Asia, Australia, America and Africa.
|
Thalidomide advertisement, 1959 |
THE TRAGEDY OF THALIDOMIDE
During the 1950’s scientists were not aware that drugs could cross the placenta and therefore thalidomide was not tested on pregnant mammals to investigate any possible adverse effects on foetal development. Within a few years, reports of children born with severe teratogenic deformities, including phocomelia, deformed eyes, and malformations of internal organs, began to surface. In 1961, an obstetrician named William McBride noted the large number of birth defects in children of mothers who were taking thalidomide during pregnancy. In December 1961, Dr. McBride had a letter published in The Lancet illustrating his findings. Around the same time, a physician named Widukind Lenz suspected thalidomide to be the cause of an outbreak of limb and ear malformation in Western Germany. Thalidomide was subsequently withdrawn from many British, Australian and West German markets however it continued to be sold for many months in other countries, including Brazil, Canada and Japan while concurrently many independent investigations confirmed thalidomide was the cause of the outbreak of children born with severe teratogenic deformities. In all it was estimated 10,000 children suffered from phocomelia as a result of thalidomide treatment, of which less than half survived due to the severity of their deformities.

|
Children exposed to thalidomide during fetal development due to maternal ingestion |
MECHANISM OF TOXICITY
|
Investigators have been studying thalidomide for 55 years now and over 30 theories have been hypothesised to account for its teratogenic effects. There is no widespread consensus on which is correct although models that implicate anti-angiogenesis and oxidative stress as responsible for the drug’s teratogenic effects have gained most widespread support. However for many years the direct molecular target and molecular mechanism of thalidomide toxicity has remained elusive. A possible mechanism suggested in 2000 by researchers is that thalidomide, or a metabolic derivative, specifically binds to GC promoter sites on IGF-1, FGF-2, αv, and β3 genes which results in decreased transcription of the associated genes. IGF-1 (insulin-like growth factor 1) and FGF-2 (fibroblast growth factor 2) stimulate the transcription of αv and β3 genes, which dimerise and stimulate angiogenesis in the developing limb bud. This promotes limb out-growth however the interaction with thalidomide disrupts normal angiogenesis, which results in truncation of the limb.
|

Relationship between several proteins, whose syntheses are potentially sensitive to thalidomide
|
alternative Mechanism
 Cereblon molecule
Cereblon molecule
A more recent investigation by Japanese researchers in 2012 implicated cereblon, a protein with an essential role in development, as the target of thalidomide’s teratogenic action. Cereblon forms an E3 ubiquitin ligase complex with other proteins which is essential for the efficient expression of fibroblast growth factor 8 (FGF8), an important regulator of limb development. However the results of the investigation suggested that thalidomide binds to cereblon, preventing the formation of E3 ubiquitin ligase and therefore downregulating FGF8 expression, resulting in limb malformation. Cereblon was implicated as thalidomide's target as in the presence of a mutant of cereblon which does not bind thalidomide, the teratogenic effects of thalidomide were suppressed in zebrafish and chicks.

|
Zebrafish (left) and chick (right) embryos that have a mutant form of cereblon. The teratogenic effects of thalidomide are suppressed. |
However this finding has not been fully accepted as another report has indicated pomalidomide does not cause teratogenic effects in these same model systems despite the fact that it causes greater inhibition of cereblon’s activity than thalidomide. Therefore there is still no widespread consensus on the direct molecular target and molecular mechanism of thalidomide toxicity.
Lessons learnt
There were many errors that led to the thalidomide scandal. In the aftermath, more structured and stricter drug regulations and control over drug use and development were implemented in many countries, including more through toxicity testing implementation of testing on pregnant mammals to identify possible developmental toxicity. All these measures have been enacted to ensure the horrors of the thalidomide crisis never occur again.

|
Suit designed for victim of thalidomide’s toxic effects |
OLD DRUG, NEW USES
 Modern thalidomide pills with printed warning against use during pregnancy
Modern thalidomide pills with printed warning against use during pregnancy
Today thalidomide is used an as an anti-cancer drug due to its anti-angiogenic activity, particularly in cases of multiple melanoma, and, in Brazil, to treat erythema nodosum leprosum (ENL), a complication of leprosy. Strict regulations accompany prescription and use of the drug such as the required use of two forms of contraception and regular pregnancy tests. However WHO do not recommend thalidomide use as “experience has shown that it is virtually impossible to develop and implement a fool-proof surveillance mechanism to combat misuse of the drug”. Unfortunately, the horrors of thalidomide continue into the 21st century, as cases of thalidomide embryopathy continue, with at least 100 cases identified in Brazil between 2005 and 2010.
